
Page 1 - Voiding Diary
P. 1
Urological Health
Voiding diary
Your name Your date of birth
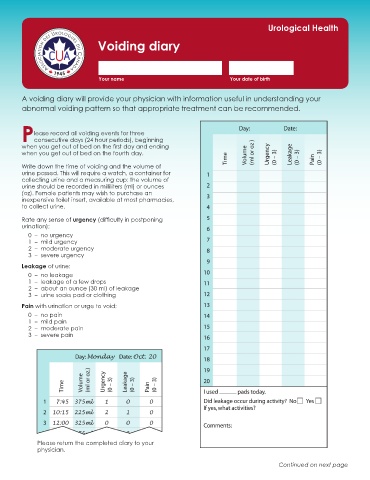
A voiding diary will provide your physician with information useful in understanding your
abnormal voiding pattern so that appropriate treatment can be recommended.
lease record all voiding events for three
Pconsecutive days (24 hour periods), beginning
when you get out of bed on the first day and ending
when you get out of bed on the fourth day.
Write down the time of voiding and the volume of
urine passed. This will require a watch, a container for
collecting urine and a measuring cup: the volume of
urine should be recorded in milliliters (ml) or ounces
(oz). Female patients may wish to purchase an
inexpensive toilet insert, available at most pharmacies,
to collect urine.
Rate any sense of urgency (difficulty in postponing
urination):
0 – no urgency
1 – mild urgency
2 – moderate urgency
3 – severe urgency
Leakage of urine:
0 – no leakage
1 – leakage of a few drops
2 – about an ounce (30 ml) of leakage
3 – urine soaks pad or clothing
Pain with urination or urge to void:
0 – no pain
1 – mild pain
2 – moderate pain
3 – severe pain
Please return the completed diary to your
physician.
Continued on next page