
Page 8 - SLIDES
P. 8
678P: Cytoreductive nephrectomy (CN) for patients with metastatic sarcomatoid and/or rhabdoid (S/R)
renal cell carcinoma (RCC) treated with immune checkpoint inhibitors (ICI)
1
1
Andrew W. Hahn , Paul V. Viscuse , Alberto C. Pieretti , Andrew J. Wiele , Eric Jonasch , Jianjun Gao , Amado J. Zurita , Amishi Y. Shah , Matthew T. Campbell ,
1
1
1
1
1
1
1
1
1
1
Padmanee Sharma , Christopher G. Wood , Nizar M. Tannir , Jose A. Karam , Pavlos Msaouel 1
1
1 The University of Texas M.D. Anderson Cancer Center, Houston, TX
• Results
Introduction Results Conclusions
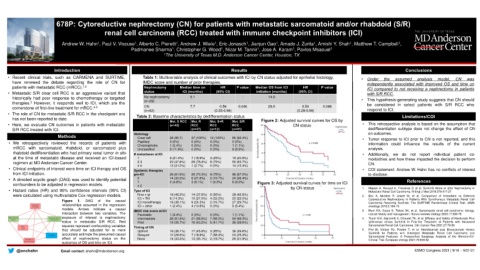
• Recent clinical trials, such as CARMENA and SURTIME, Table 1: Multivariable analysis of clinical outcomes with ICI by CN status adjusted for epithelial histology, • Under the assumed analysis model, CN was
have renewed the debate regarding the role of CN for IMDC score and number of prior therapies. independently associated with improved OS and time on
patients with metastatic RCC (mRCC). 1,2 Nephrectomy Median time on HR P value Median OS from ICI HR P value ICI compared to not receiving a nephrectomy in patients
• Metastatic S/R clear cell RCC is an aggressive variant that status ICI (months) (95% CI) initiation (months) (95% CI) with S/R RCC.
historically had poor response to chemotherapy or targeted No nephrectomy 5.1 - - 14.0 - - • This hypothesis-generating study suggests that CN should
therapies. However, it responds well to ICI, which are the (n=29) be considered in select patients with S/R RCC who
3
cornerstone of first-line treatment for mRCC. 4-5 CN 7.7 0.59 0.046 29.0 0.54 0.048 respond to ICI.
(n=62)
(0.35-0.99)
• The role of CN for metastatic S/R RCC in the checkpoint era Table 2: Baseline characteristics by dedifferentiation status (0.29-0.99) Limitations/COI
has not been reported to date.
Met. S RCC Met. R Met. S+R Met. S/R Figure 2: Adjusted survival curves for OS by
• Here, we evaluate CN outcomes in patients with metastatic (n=42) RCC RCC RCC CN status • This retrospective analysis is based on the assumption that
S/R RCC treated with ICI. (n=37) (n=12) (n=91) dedifferentiation subtype does not change the effect of CN
Histology on outcomes.
Methods Clear cell 36 (85.7) 37 (100%) 12 (100%) 85 (93.4%) • Tumor response to ICI prior to CN is not reported, and this
• We retrospectively reviewed the records of patients with Papillary 0 (0%) 0 (0%) 0 (0%) 0 (0%) information could influence the results of the current
Chromophobe
1 (2.4%)
0 (0%)
AV
1 (1.1%)
0 (0%)
mRCC with sarcomatoid, rhabdoid, or sarcomatoid plus Unclassified 5 (11.9%) 0 (0%) 0 (0%) 5 (5.5%) analysis.
rhabdoid dedifferentiation who had primary renal tumor in situ # metastases at ICI • Additionally, we do not report individual patient co-
at the time of metastatic disease and received an ICI-based 1 9 (21.4%) 7 (18.9%) 3 (25%) 19 (20.9%) morbidities and how these impacted the decision to perform
regimen at MD Anderson Cancer Center. 2-3 20 (47.6%) 29 (78.4%) 9 (75%) 58 (63.7%) CN.
≥ 4 13 (31.0%) 1 (2.7%) 0 (0%) 14 (15.4%)
• Clinical endpoints of interest were time on ICI therapy and OS Systemic therapies • COI statement: Andrew W. Hahn has no conflicts of interest
from ICI initiation. pre-ICI 26 (61.9%) 26 (70.3%) 9 (75%) 96 (67.0%) to disclose.
• A directed acyclic graph (DAG) was used to identify potential 0 1 14 (33.3%) 8 (21.6%) 2 (16.7%) 24 (26.4%) References
3 (8.1%)
6 (6.6%)
1 (8.3%)
2 (4.8%)
confounders to be adjusted in regression models. ≥ 2 Figure 3: Adjusted survival curves for time on ICI
• Hazard ratios (HR) and 95% confidence intervals (95% CI) Type of ICI by CN status 1. Mejean A, Ravaud A, Thezenas S, et al. Sunitinib Alone or after Nephrectomy in
Metastatic Renal-Cell Carcinoma. N Engl J Med 2018;379:417-27.
were calculated using multivariable Cox regression models. Nivo + ipi 19 (45.2%) 14 (37.8%) 6 (50%) 39 (42.9%) 2. Bex A, Mulders P, Jewett M, et al. Comparison of Immediate vs Deferred
Figure 1. DAG of the causal ICI + TKI 6 (14.3%) 10 (27.0%) 4 (33.3%) 20 (22.0%) Cytoreductive Nephrectomy in Patients With Synchronous Metastatic Renal Cell
9 (24.3%)
27 (29.7%)
ICI monotherapy
2 (16.7%)
16 (38.1%)
Carcinoma Receiving Sunitinib: The SURTIME Randomized Clinical Trial. JAMA
relationships assumed in the regression ICI + other 1 (2.4%) 4 (10.8%) 0 (0%) 5 (5.4%) oncology 2019;5:164-70.
models. Arrows indicate a causal IMDC risk score at ICI 3. Blum KA, Gupta S, Tickoo SK, et al. Sarcomatoid renal cell carcinoma: biology,
interaction between two variables. The Favorable 1 (2.4%) 0 (0%) 0 (0%) 1 (1.1%) natural history and management. Nature reviews Urology 2020;17:659-78
exposure of interest is nephrectomy Intermediate 26 (61.9%) 21 (56.8%) 7 (58.3%) 54 (59.3%) 4. Tannir NM, Signoretti S, Choueiri TK, et al. Efficacy and Safety of Nivolumab Plus
status in metastatic S/R RCC. Red Poor 15 (35.7%) 16 (43.2%) 5 (41.7%) 36 (39.6%) Ipilimumab versus Sunitinib in First-line Treatment of Patients with Advanced
squares represent confounding variables Timing of CN Sarcomatoid Renal Cell Carcinoma. Clin Cancer Res 2021;27:78-86
that should be adjusted for to more Upfront 16 (38.1%) 17 (45.9%) 3 (25%) 36 (39.6%) 5. Rini BI, Motzer RJ, Powles T, et al. Atezolizumab plus Bevacizumab Versus
accurately estimate the presumed causal Delayed 12 (28.6%) 7 (18.9%) 7 (58.3%) 23 (25.3%) Sunitinib for Patients with Untreated Metastatic Renal Cell Carcinoma and
Sarcomatoid Features: A Prespecified Subgroup Analysis of the IMmotion151
effect of nephrectomy status on the None 14 (33.3%) 13 (35.1%) 2 (16.7%) 29 (31.9%) Clinical Trial. European urology 2021;79:659-62
outcomes of OS and time on ICI.
@onchahn Email contact: ahahn@mdanderson.org ESMO Congress 2021 | 9/16 – 9/21/21