
Page 2 - PSA Screening Pocket Guide 2021
P. 2
A Practical Approach to the Canadian Urological Association
Recommendations on Prostate Cancer Screening and Early Diagnosis 1
PSA Screening
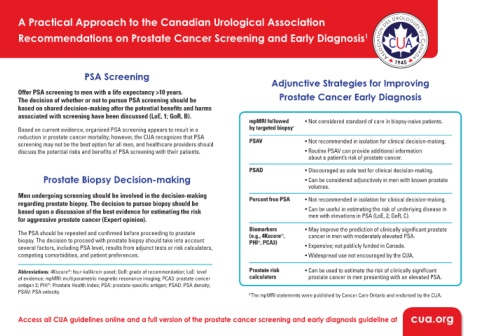
Adjunctive Strategies for Improving
Offer PSA screening to men with a life expectancy >10 years. Prostate Cancer Early Diagnosis
The decision of whether or not to pursue PSA screening should be
based on shared decision-making after the potential benefits and harms
associated with screening have been discussed (LoE, 1; GoR, B).
mpMRI followed • Not considered standard of care in biopsy-naive patients.
Based on current evidence, organized PSA screening appears to result in a by targeted biopsy *
reduction in prostate cancer mortality; however, the CUA recognizes that PSA
screening may not be the best option for all men, and healthcare providers should PSAV • Not recommended in isolation for clinical decision-making.
discuss the potential risks and benefits of PSA screening with their patients. • Routine PSAV can provide additional information
about a patient’s risk of prostate cancer.
PSAD • Discouraged as sole test for clinical decision-making.
Prostate Biopsy Decision-making • Can be considered adjunctively in men with known prostate
volumes.
Men undergoing screening should be involved in the decision-making Percent free PSA • Not recommended in isolation for clinical decision-making.
regarding prostate biopsy. The decision to pursue biopsy should be
based upon a discussion of the best evidence for estimating the risk • Can be useful in estimating the risk of underlying disease in
men with elevations in PSA (LoE, 2; GoR, C).
for aggressive prostate cancer (Expert opinion).
Biomarkers • May improve the prediction of clinically significant prostate
The PSA should be repeated and confirmed before proceeding to prostate (e.g., 4Kscore , cancer in men with moderately elevated PSA.
®
biopsy. The decision to proceed with prostate biopsy should take into account PHI , PCA3)
®
several factors, including PSA level, results from adjunct tests or risk calculators, • Expensive; not publicly funded in Canada.
competing comorbidities, and patient preferences. • Widespread use not encouraged by the CUA.
Abbreviations: 4Kscore : four-kallikrein panel; GoR: grade of recommendation; LoE: level Prostate risk • Can be used to estimate the risk of clinically significant
®
of evidence; mpMRI: multiparametric magnetic resonance imaging; PCA3: prostate cancer calculators prostate cancer in men presenting with an elevated PSA.
antigen 3; PHI : Prostate Health Index; PSA: prostate-specific antigen; PSAD: PSA density;
®
PSAV: PSA velocity.
*The mpMRI statements were published by Cancer Care Ontario and endorsed by the CUA.
Access all CUA guidelines online and a full version of the prostate cancer screening and early diagnosis guideline at cua.org