
Page 45 - Flipbook
P. 45
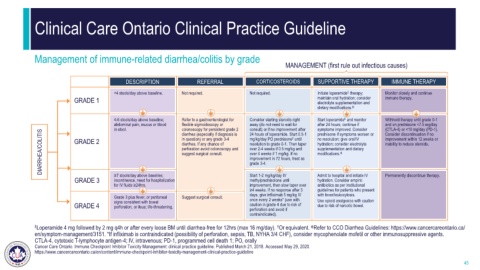
Clinical Care Ontario Clinical Practice Guideline
Management of immune-related diarrhea/colitis by grade
MANAGEMENT (first rule out infectious causes)
DESCRIPTION REFERRAL CORTICOSTEROIDS SUPPORTIVE THERAPY IMMUNE THERAPY
<4 stools/day above baseline. Not required. Not required. Initiate loperamide therapy; Monitor closely and continue
£
GRADE 1 maintain oral hydration; consider immune therapy.
electrolyte supplementation and
dietary modifications. ф
4-6 stools/day above baseline; Refer to a gastroenterologist for Consider starting steroids right Start loperamide and monitor Withhold therapy until grade 0-1
£
abdominal pain, mucus or blood flexible sigmoidoscopy or away (do not need to wait for after 24 hours; continue if and on prednisone <7.5 mg/day
in stool. colonoscopy for persistent grade 2 consult) or if no improvement after symptoms improved. Consider (CTLA-4) or <10 mg/day (PD-1).
DIARRHEA/COLITIS GRADE 2 diarrhea. If any chance of resolution to grade 0-1. Then taper hydration; consider electrolyte inability to reduce steroids.
diarrhea (especially if diagnosis is
Consider discontinuation if no
24 hours of loperamide. Start 0.5-1
prednisone if symptoms worsen or
improvement within 12 weeks or
no resolution; give oral/IV
†
mg/kg/day PO prednisone until
in question) or any grade 3-4
supplementation and dietary
over 2-4 weeks if 0.5 mg/kg and
perforation avoid colonoscopy and
modifications.
over 4 weeks if 1 mg/kg. If no
suggest surgical consult.
ф
improvement in 72 hours, treat as
grade 3-4.
GRADE 3 ≥7 stools/day above baseline; Start 1-2 mg/kg/day IV Admit to hospital and initiate IV Permanently discontinue therapy.
incontinence, need for hospitalization
methylprednisolone until
hydration. Consider empiric
for IV fluids ≥24hrs. improvement, then slow taper over antibiotics as per institutional
≥4 weeks. If no response after 3 guidelines for patients who present
days, give infliximab 5 mg/kg IV with fever/leukocytosis.
Grade 3 plus fever, or peritoneal Suggest surgical consult. once every 2 weeks* (use with Use opioid analgesics with caution
GRADE 4 signs consistent with bowel caution in grade 4 due to risk of due to risk of narcotic bowel.
perforation, or ileus; life-threatening.
perforation and avoid if
contraindicated).
ф
£ Loperamide 4 mg followed by 2 mg q4h or after every loose BM until diarrhea-free for 12hrs (max 16 mg/day). Or equivalent. Refer to CCO Diarrhea Guidelines: https://www.cancercareontario.ca/
†
en/symptom-management/3151. *If infliximab is contraindicated (possibility of perforation, sepsis, TB, NYHA 3/4 CHF), consider mycophenolate mofetil or other immunosuppressive agents.
CTLA-4, cytotoxic T-lymphocyte antigen-4; IV, intravenous; PD-1, programmed cell death 1; PO, orally
Cancer Care Ontario. Immune Checkpoint Inhibitor Toxicity Management: clinical practice guideline. Published March 21, 2018. Accessed May 29, 2020.
https://www.cancercareontario.ca/en/content/immune-checkpoint-inhibitor-toxicity-management-clinical-practice-guideline
45