
Page 25 - PACE: Advanced Prostate Cancer Consensus
P. 25
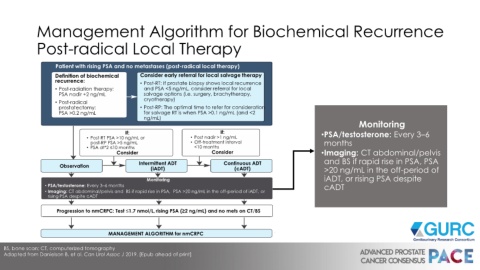
Management Algorithm for Biochemical Recurrence
Post-radical Local Therapy
Patient with rising PSA and no metastases (post-radical local therapy)
Definition of biochemical Consider early referral for local salvage therapy
recurrence: • Post-RT: If prostate biopsy shows local recurrence
• Post-radiation therapy: and PSA <5 ng/mL, consider referral for local
PSA nadir +2 ng/mL salvage options (i.e. surgery, brachytherapy,
• Post-radical cryotherapy)
prostatectomy: • Post-RP: The optimal time to refer for consideration
PSA >0.2 ng/mL for salvage RT is when PSA >0.1 ng/mL (and <2
ng/mL)
Monitoring
If: If: •PSA/testosterone: Every 3–6
• Post-RT PSA >10 ng/mL or • Post nadir >1 ng/mL
post-RP PSA >5 ng/mL • Off-treatment interval months
• PSA dt*2 ≤10 months <10 months
Consider Consider •Imaging: CT abdominal/pelvis
Observation Intermittent ADT Continuous ADT and BS if rapid rise in PSA, PSA
(iADT) (cADT) >20 ng/mL in the off-period of
Monitoring iADT, or rising PSA despite
• PSA/testosterone: Every 3–6 months cADT
• Imaging: CT abdominal/pelvis and BS if rapid rise in PSA, PSA >20 ng/mL in the off-period of iADT, or
rising PSA despite cADT
Progression to nmCRPC: Test ≤1.7 nmol/L, rising PSA (≥2 ng/mL) and no mets on CT/BS
MANAGEMENT ALGORITHM for nmCRPC
BS, bone scan; CT, computerized tomography
Adapted from Danielson B, et al. Can Urol Assoc J 2019. [Epub ahead of print]