
Page 23 - August 2022_Fulldraftforflipbook_revised
P. 23
CUA guideline: LUTS/BPH
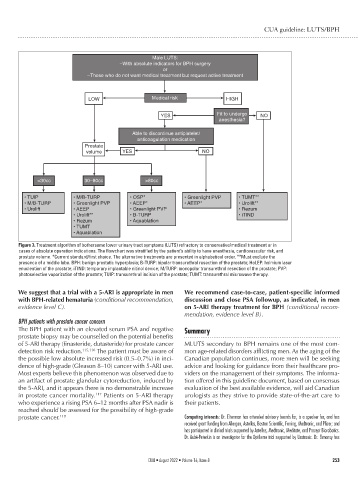
Male LUTS:
–With absolute indicators for BPH surgery
or
–Those who do not want medical treatment but request active treatment
LOW Medical risk HIGH
Fit to undergo
YES NO
anesthesia?
Able to discontinue antiplatelet/
anticoagulation medication
Prostate
volume YES NO
<30cc 30–80cc >80cc
• TUIP • M/B-TURP • OSP* • Greenlight PVP • TUMT**
• M/B-TURP •Greenlight PVP • AEEP* • AEEP* • Urolift**
• Urolift • AEEP • Greenlight PVP • Rezum
• Urolift** • B-TURP • iTIND
• Rezum • Aquablation
• TUMT
• Aquablation
Figure 3. Treatment algorithm of bothersome lower urinary tract symptoms (LUTS) refractory to conservative/medical treatment or in
cases of absolute operation indications. The flowchart was stratified by the patient’s ability to have anesthesia, cardiovascular risk, and
prostate volume. *Current standard/first choice. The alternative treatments are presented in alphabetical order. **Must exclude the
presence of a middle lobe. BPH: benign prostatic hyperplasia; B-TURP: bipolar transurethral resection of the prostate; HoLEP: holmium laser
enucleation of the prostate; iTIND: temporary implantable nitinol device; M/TURP: monopolar transurethral resection of the prostate; PVP:
photoselective vaporization of the prostate; TUIP: transurethral incision of the prostate; TUMT: transurethral microwave therapy.
We suggest that a trial with a 5-ARI is appropriate in men We recommend case-to-case, patient-specific informed
with BPH-related hematuria (conditional recommendation, discussion and close PSA followup, as indicated, in men
evidence level C). on 5-ARI therapy treatment for BPH (conditional recom-
mendation, evidence level B).
BPH patients with prostate cancer concern
The BPH patient with an elevated serum PSA and negative Summary
prostate biopsy may be counselled on the potential benefits
of 5-ARI therapy (finasteride, dutasteride) for prostate cancer MLUTS secondary to BPH remains one of the most com-
detection risk reduction. 115,116 The patient must be aware of mon age-related disorders afflicting men. As the aging of the
the possible low absolute increased risk (0.5–0.7%) in inci- Canadian population continues, more men will be seeking
dence of high-grade (Gleason 8–10) cancer with 5-ARI use. advice and looking for guidance from their healthcare pro-
Most experts believe this phenomenon was observed due to viders on the management of their symptoms. The informa-
an artifact of prostate glandular cytoreduction, induced by tion offered in this guideline document, based on consensus
the 5-ARI, and it appears there is no demonstrable increase evaluation of the best available evidence, will aid Canadian
in prostate cancer mortality. 117 Patients on 5-ARI therapy urologists as they strive to provide state-of-the-art care to
who experience a rising PSA 6–12 months after PSA nadir is their patients.
reached should be assessed for the possibility of high-grade
prostate cancer. 118 Competing interests: Dr. Elterman has attended advisory boards for, is a speaker for, and has
received grant funding from Allergan, Astellas, Boston Scientific, Ferring, Medtronic, and Pfizer; and
has participated in clinical trials supported by Astellas, Medtronic, Meditate, and Procept Biorobotics.
Dr. Aubé-Peterkin is an investigator for the Optilume trial supported by Urotronic. Dr. Elmansy has
CUAJ • August 2022 • Volume 16, Issue 8 253