
Page 3 - CUA Best Practice Report: Pediatric hemorrhagic cystitis
P. 3
BPR: Pediatric hemorrhagic cystitis
is associated with a greater risk of mortality, particularly if or diffusely increased in the setting of HC. Doppler investi-
20
HC presents before 200 days post-SCT (p=0.002). Viral eti- gation may also reveal focal or diffuse hypervascularity, as
ology did not affect post-SCT survival, rather hematological well as distinct bleeding, which may be amenable to targeted
malignancy (OR 2.74) and ifosfamide exposure (OR 1.988) cautery during cystoscopic evaluation.
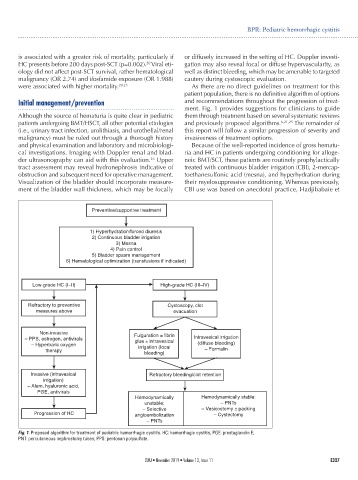
were associated with higher mortality. 20,23 As there are no direct guidelines on treatment for this
patient population, there is no definitive algorithm of options
Initial management/prevention and recommendations throughout the progression of treat-
ment. Fig. 1 provides suggestions for clinicians to guide
Although the source of hematuria is quite clear in pediatric them through treatment based on several systematic reviews
patients undergoing BMT/HSCT, all other potential etiologies and previously proposed algorithms. 6,21,25 The remainder of
(i.e., urinary tract infection, urolithiasis, and urothelial/renal this report will follow a similar progression of severity and
malignancy) must be ruled out through a thorough history invasiveness of treatment options.
and physical examination and laboratory and microbiologi- Because of the well-reported incidence of gross hematu-
cal investigations. Imaging with Doppler renal and blad- ria and HC in patients undergoing conditioning for alloge-
der ultrasonography can aid with this evaluation. Upper neic BMT/SCT, these patients are routinely prophylactically
26
tract assessment may reveal hydronephrosis indicative of treated with continuous bladder irrigation (CBI), 2-mercap-
obstruction and subsequent need for operative management. toethanesulfonic acid (mesna), and hyperhydration during
Visualization of the bladder should incorporate measure- their myelosuppressive conditioning. Whereas previously,
ment of the bladder wall thickness, which may be focally CBI use was based on anecdotal practice, Hadjibabaie et
Preventive/supportive treatment
1) Hyperhydration/forced diuresis
2) Continuous bladder irrigation
3) Mesna
4) Pain control
5) Bladder spasm management
6) Hematological optimization (transfusions if indicated)
Low-grade HC (I–II) High-grade HC (III–IV)
Refractory to preventive Cystoscopy, clot
measures above evacuation
Non-invasive Fulguration ± fibrin
– PPS, estrogen, antivirals Intravesical irrigation
glue ± intravesical
– Hyperbaric oxygen irrigation (focal (diffuse bleeding)
therapy – Formalin
bleeding)
Invasive (intravesical Refractory bleeding/clot retention
irrigation)
– Alum, hyaluronic acid,
PGE, antivirals
Hemodynamically Hemodynamically stable:
unstable: – PNTs
– Selective – Vesicostomy ± packing
Progression of HC angioembolization – Cystectomy
– PNTs
Fig. 1. Proposed algorithm for treatment of pediatric hemorrhagic cystitis. HC: hemorrhagic cystitis; PGE: prostaglandin E;
PNT: percutaneous nephrostomy tubes; PPS: pentosan polysulfate.
CUAJ • November 2019 • Volume 13, Issue 11 E327